For patients that have had a breast removed from cancer or other disease, breast reconstruction is a surgical option. This can be performed at the same time as the breast is being removed or in a delayed fashion.
There are several reconstructive options available. The most common reconstructions are skin expansion and flap reconstruction. With skin expansion, a balloon expander is placed beneath the skin and chest muscle. This is gradually filled over several weeks or months. This expander is eventually replaced with either a silicone or saline implant. Some expanders are designed to be left in place as the final implant. In flap reconstruction, tissue is moved from another site of the body to the chest to form a new breast. Tissue can be taken from the abdomen and tunneled beneath the skin to form a new breast mound (TRAM flap). Alternatively, tissue can be taken from the back to reconstruct the breast (latissimus flap). These procedures usually require inpatient hospital stays and are typically covered by insurance as required by the 1998 federal breast reconstruction law.
Procedural Steps
First, Anesthesia is induced
Medications are administered for your comfort during the surgical procedure. This procedure is usually done under general anesthesia
Breast reconstruction with Tissue expander
With this type of reconstruction, a balloon expander is placed beneath the skin and chest muscle. This is gradually filled over several months.
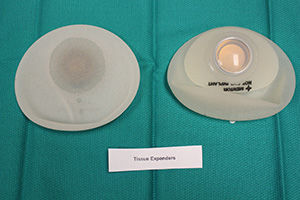
This expander is eventually replaced with either a silicone or saline implant.
Reconstruction with tissue expansion allows an easier recovery than flap procedures, but it is a more lengthy reconstruction process.
It requires many office visits over 4-6 months after placement of the expander to slowly fill the device through an internal valve to expand the skin.
A second surgical procedure will be needed to replace the expander if it is not designed to serve as a permanent implant.
In certain situations, the expansion phase can be eliminated and a silicone or saline implant can be placed in one surgery (called direct to implant reconstruction)
Breast reconstruction is completed through a variety of techniques that reconstruct the nipple and areola.
Implant Choices
Saline breast implants
Are filled with sterile salt water. Should the implant shell leak, a saline implant will collapse and the saline will be absorbed and naturally expelled by the body.
Saline breast implants provide a uniform shape, firmness and feel.
Silicone breast implants
Are filled with silicone gel. The gel feels a bit more like natural breast tissue. If the implant leaks, the gel may remain within the implant shell, or may escape into the breast implant pocket. A leaking implant filled with silicone gel will not collapse.
If you choose silicone implants, you may need to visit your plastic surgeon regularly to make sure the implants are functioning properly. An ultrasound or MRI screening can assess the condition of breast implants.
Form-stable implants
Are sometimes referred to as gummy bear breast implants because they maintain their shape even when the implant shell is broken.
The consistency of the silicone gel inside the implant is thicker than traditional silicone gel implants. These implants are also firmer than traditional implants, but are thought to be less likely to break.
Gummy bear breast implants are shaped rather than round. They have more projection at the bottom and are tapered towards the top. If a shaped implant rotates, it may lead to an unusual appearance of the breast.
Placement of gummy bear implants requires a longer incision in the skin.
Additional Methods
Latissimus Flap
A latissimus dorsi flap uses muscle, fat and skin from the back tunneled to the mastectomy site and remains attached to its donor site, leaving blood supply intact. Occasionally, the flap can reconstruct a complete breast mound, but often provides the muscle and tissue necessary to cover and support a breast implant or tissue expander.
The latissimus dorsi flap is often used as a backup option if a patient has wound healing problems or soft tissue failure in the setting of an implant. The latissimus dorsi flap can also be used as a salvage procedure for patients who have had previous radiation. A large open wound on the chest wall is also an indication for an LD flap in patients that need chest wall reconstruction alone, without creation of a breast shape.
The length of surgery for latissimus dorsi flap breast reconstruction is typically about 4 hours, and usually requires 1-2 day hospital stay. The initial recovery time is two to three weeks. Patients generally have no major long-term physical limitations from taking the latissimus muscle. Activities of daily living and most exercise can be resumed without significant loss of proficiency.
Secondary procedures after an latissimus dorsi flap reconstruction can be done in about three months. These may include expander implant exchange, adjustment procedures to improve breast symmetry, and nipple areola reconstruction. As with any type of reconstruction, if chemotherapy is needed, any additional surgery must await completion of treatment. Such additional procedures are typically done as outpatient surgery.
You may be a candidate for latissimus dorsi flap reconstruction if you:
- are thin with a small breast volume
- have excess tissue laterally and upward across the midback
- have had previous radiation and are having an implant reconstruction
- have thin skin that requires extra coverage for an implant
- are having immediate or delayed reconstruction
You may not be an ideal candidate for a latissimus dorsi flap reconstruction if you:
- do not wish to have additional scarring to a part of the body other than the breasts
- have had previous chest-wall surgery such as a thoracotomy
- participate in extreme competitive sports such as mountain climbing, skiing, and swimming
TRAM Flap
Uses donor muscle, fat and skin from a woman’s abdomen to reconstruct the breast. The flap may either remain attached to the original blood supply and be tunneled up through the chest wall, or be completely detached, and formed into a breast mound.
The TRAM flap operation is more involved than implant reconstruction. The length of surgery for a unilateral TRAM flap reconstruction is about 5 hours. For bilateral reconstruction, it can take 6-8 hours. The hospital stay is usually 3-5 days. You may have abdominal pain and tightness for several weeks, and it can often take several months to return to a full range of activity.
While the benefit of a TRAM flap is using your own tissue, the primary disadvantages relate to the length of surgery, the long recovery and the abdominal wall donor site. This includes potential abdominal wall weakness, bulging, and hernia. To prevent hernia, a synthetic mesh may have to be used when closing the abdomen.
Secondary procedures after a TRAM flap reconstruction can be done in about 3 months. However, if chemotherapy is needed, any additional surgery must await completion of treatment. At that point, the patient can have revisions to the breasts and abdomen, and the nipple and areola can be created. Such additional procedures are typically done as outpatient surgery.
You may be a candidate for TRAM flap reconstruction if you:
- desire autogeneous reconstruction
- do not want or are not a candidate for implant reconstruction
- have enough lower abdominal wall tissue to create one or both breasts
- have not had prior abdominal surgery
- have had previous chest wall radiation
- have had failed implant reconstruction
You are not an ideal candidate for TRAM flap reconstruction if you:
- do not have enough lower abdominal tissue to create the flaps
- have a large overhanging pannus of abdominal skin and fat
- have a BMI of 30 or above
- have diabetes
- are a smoker or quit smoking only recently
- have had previous abdominal surgeries such as abdominoplasty
- cannot tolerate anesthesia for long periods
- do not wish to have a lower abdominal scar
Breast reconstruction recovery
Following your breast reconstruction surgery by flap techniques and/or the insertion of a breast implant, gauze or bandages will be applied to your incisions.
A small, thin tube may be temporarily placed under the skin to drain any excess blood or fluid.
You will be given specific instructions that may include: How to care for your surgical site(s) following surgery, medications to apply or take orally to aid healing and reduce the risk of infection, specific concerns to look for at the surgical site or in your general health, and when to follow up in the office.
Breast reconstruction risks and safety information
The decision to have breast reconstruction surgery is extremely personal. You’ll have to decide if the benefits will achieve your goals and if the risks and potential complications are acceptable.
At your initial consult, we will explain in detail the risks associated with surgery. You will be asked to sign consent forms to ensure that you fully understand the procedures you will undergo and any risks or potential complications.
The possible risks of breast reconstruction include, but are not limited to, bleeding, infection, poor healing of incisions, and anesthesia risks. You should also know that:
- Flap surgery includes the risk of partial or complete loss of the flap and a loss of sensation at both the donor and reconstruction site.
- The use of implants carries the risk of breast firmness (capsular contracture) and implant rupture.
Breast implants do not impair breast health. Careful review of scientific research conducted by independent groups such as the Institute of Medicine has found no proven link between breast implants and autoimmune or other systemic diseases. Visit breastimplantsafety.org for current information.